Isthmus Gifts
April 1, 2022
By Lisa Germain, DDS, MScD
The construction of the Panama Canal, which created a water passage from the Atlantic to the Pacific Ocean, was a difficult and lengthy process. Early explorers of the Americas and European colonists of central America recognized the potential, but it was not attempted until technological advances allowed first France, and then ultimately the United States to carry out the deep excavations necessary to complete the project. Opened in 1914, and still in operation today, it cuts across the Isthmus of Panama serving as an important conduit of international maritime trade. In a parallel world in the early 20th century, dentists were exploring a different type of canal system. It appeared that human teeth had much more intricate passage ways between the roots than originally thought.
In 1927 Walter Hess published a study detailing the “purely anatomical conditions in the root-canals of human teeth”. He cleared and sectioned twenty-eight hundred specimens obtained from people ages five to fifty-five years old. These teeth did not have prior pulp extirpation. His study confirmed previous theories that root canals are complex and he wrote: “a thorough knowledge of them is important”. 1 The images he showed brought to the forefront in endodontics an awareness of the complex interconnections of the root canal system, as well as the challenges of not having the necessary technological advances to negotiate them. He did not have the advantage of CBCT technology that assists us today.
Derived from the Greek word isthmos, the isthmus as defined by Weller et al is a narrow connection between two root canals that contains pulp tissue. 2 Others have called it a transverse anastomosis (Vertucci, 1984) 3, a corridor (Green, 1973) 4, and a lateral interconnection (Pineda, 1973) 5.
Isthmuses are prevalent in all types of roots in which two or more canals are normally found. These include mandibular incisors, the maxillary and mandibular first and second premolars, the mesial roots of maxillary and mandibular molars, maxillary second molars, and the distal root of mandibular molars.6 Not all anomalies occur within the isthmus, but it is necessary to thoroughly explore this area and be aware of the anatomic variations that arise from these internal connections.
The embryonic origin of the isthmus in the root canal system is through Hertwig’s Epithelial Root Sheath. In single roots, gaps occur in dentin formation that in turn prevents cementum deposition in these areas. This leads to the formation of lateral and accessory canals most commonly observed in the apical third of the root. In multiple rooted teeth with multiple canals, these defects occur with a higher incidence and an isthmus is formed when an individual root projection is unable to close itself off. Partial fusion of the root projections result in the formation of two root canals with an isthmus formed in between, such as the distal root of the mandibular first molar. If no fusion occurs, a large ribbon shaped canal forms an isthmus throughout the entire root.7
During endodontic treatment, the tissue trapped in the ramifications between the main canals is not readily removed with instruments. Isthmus cleaning has been historically relegated to copious irrigation with appropriate solutions. 8 In earlier years intracanal medicaments such as formocresol, cresatin and CMCP [camphorated p-monochlorophenol] were relied upon to render the unreachable areas sterile. These agents were responsible for that classic “dental office smell”, and did more in the way of fumigating the canals instead of disinfecting them. Bleach is still widely considered the gold standard for canal cleaning due to its outstanding disinfectant properties, easy availability, and cost effectiveness. In addition, lubricants, chelating agents, calcium hydroxide, alcohol, peroxide, and assorted proprietary formulas, provide adjunctive methods for cleaning the complete root canal system. In recent years, various energy sources (i.e., ultrasonic devices and lasers) have shown promise as a more complete solution to this clinical dilemma and will most likely continue to be developed. Microsurgical techniques have stressed the importance of including the isthmus in the ultrasonic retro-preparation for root end filling for apicoectomy procedures. 9
Root canal anatomy varies widely between the genders and is not static over a person’s lifetime. With age, the formation of secondary dentin results in an increase in the development of cross-linking within the canals. In addition, ethnicity plays a significant role in anatomical development of the root canal space with some races having a greater number of canals than previously reported in the literature. 10,11,12
For decades, Vertucci’s classification for root canal anatomy has been used to categorize anomalous root canal systems. He noted 8 different canal system types based on the number of canals within each root and whether they had anastomosis, a common or separate orifice, and a common or separate portal of exit. 3 In 2004, Sert and Bayerili studied teeth by gender in the Turkish population and reported 14 additional types not included in the Vertucci classification. 13
Mandibular Anteriors
Using radiographs, Benjamin and Dowson studied 364 mandibular incisors and reported 41.4% of their sample had 2 separate canals, with separate foramina occurring in only 1.3% of the samples. 14 In contrast, Miyashita et al studied 1085 specimens and reported that only 3.1% had separate canals and foramina. 15 This wide variation in reported data makes endodontic treatment planning difficult. 16
Rather than relying on the statistics, the clinician should look at each tooth as having the potential for multiple interconnected canals. The mandibular anterior teeth are particularly challenging due to the small coronal tooth structure and position in the mouth, particularly if they are inclined lingually. Adequate radiographic angles should be taken if a CBCT is not available. In addition, illumination and magnification are imperative when searching for delicate anatomy. An important clinical observation is that if a root is wide buccal-lingually, it is likely to have more than one canal.
Figure 1a shows a preoperative radiograph of tooth #26 with 2 canals on a 65-year-old Caucasian male. After access was created, an isthmus was visualized in a buccal-lingual direction. The main canal was located, cleaned and shaped. The second canal was located within the isthmus under the cingulum of the tooth. Figure 1b shows a postoperative radiograph with 2 canals cleaned, shaped, and obturated in 3 dimensions.
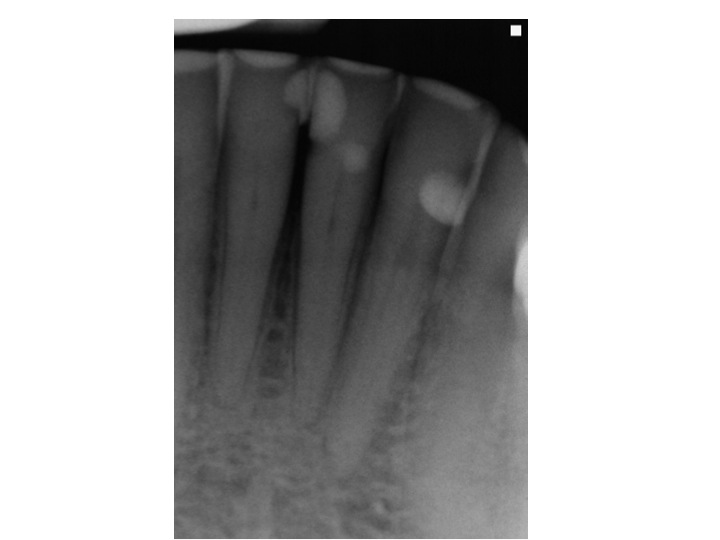
1a.: Pre-op # 26 revealing 2 canals
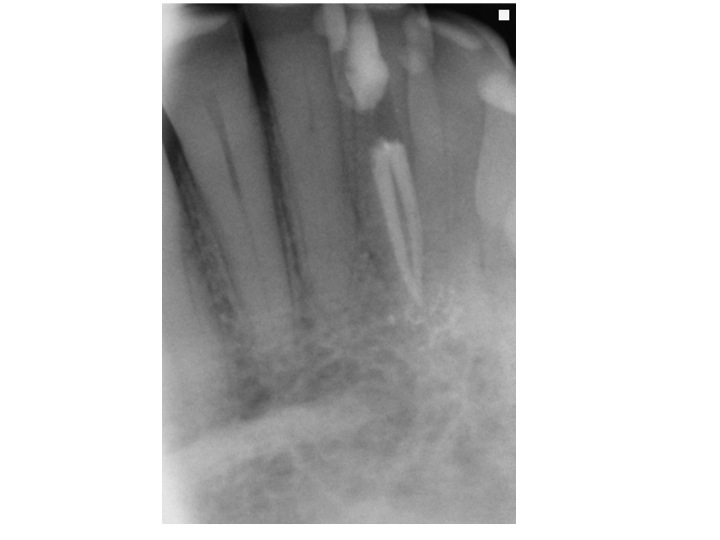
1b. Post-op #26 showing gutta percha filling of 2 canals
Premolars
Premolar teeth vary widely in their anatomy as well. Vertucci 3 described a varying number of roots with intercommunications. In maxillary first premolars, two or more canals were found in one root 30% of the time, while 41% of the maxillary second premolars had to or more canals. In addition he reported that mandibular first premolars presented with two or three canals 27% of the time, and second premolars presented with an additional canal 2% of the time. Green4 reported two orifices on the floor of the pulp chamber joined by an isthmus in 92% of maxillary first premolars, and in 28% of maxillary second premolars. In mandibular first premolars he reported two orifices in 14% of the cases and 8% in mandibular second premolars.
Figure 2a shows a preoperative radiograph of tooth #4 on a 48 -year old Asian female. Note the disappearance of a distinct canal system, which is often a clue when predicting difficult anatomy. Figure 2b shows a postoperative radiograph revealing 3 separate canals with separate terminus.

2a. Pre-op #4 with unclear anatomy from single image

2b. Post op #4: Obturation of 3 canals.
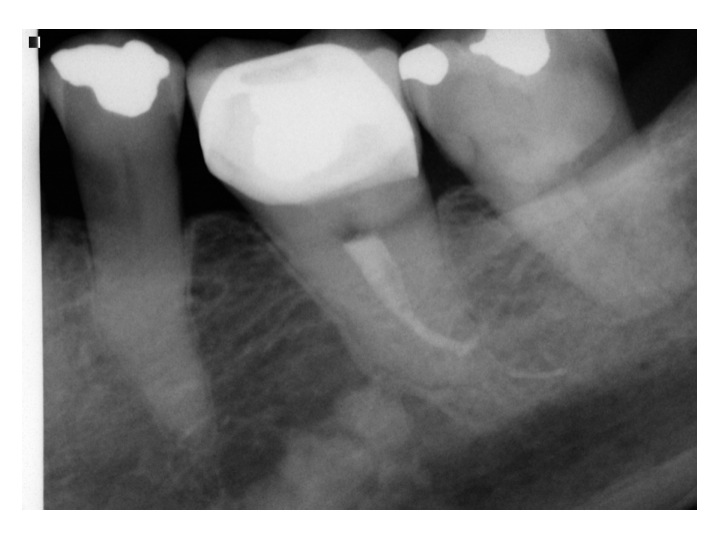
Figure 3a shows a preoperative radiograph of teeth #20 and 21 on a 52-year old African American male. In the previous root canal treatment of tooth #20, 2 canals were located, but pain persisted and was reproduced on both teeth. The radiograph of tooth #21 reveals a canal system that disappears becoming almost amorphous in nature and is indicative of the potential for a multi-rooted tooth. The final retreatment of this case can be observed in Figure 3b. Tooth #21 shows a rare 3-canal system. Even more notable is the filled isthmus in the retreatment of tooth #20 and an apical interconnection. By cleaning out the isthmus and negotiating the previously untreated canals, the symptoms resolved.

3a. Pre-op #20 and 21

3b. Post-op #20 and 21: Obturation of multiple canal systems in premolar teeth.
Molars
In 1990, Kulid and Peters 17 reported up to 95% of the mesiobuccal roots of maxillary molars have two canal systems. Many clinical articles have been written discussing cases whereby these canals were found to have an isthmus that connects them. 18 Figure 4a and 4b illustrate another common anomaly. Clinically, this maxillary second molar presents with one main ribbon shaped canal, divided by a narrow fin. Unlike most maxillary second molars whereby access to the area makes canal negotiation challenging, this type of anatomy has the benefit of being treated like a central incisor in the back of the mouth. (Talk about an isthmus gift!)

4a. Pre-op #2

4b. Post-op #2 :Obturation of a single canal in an upper second molar.
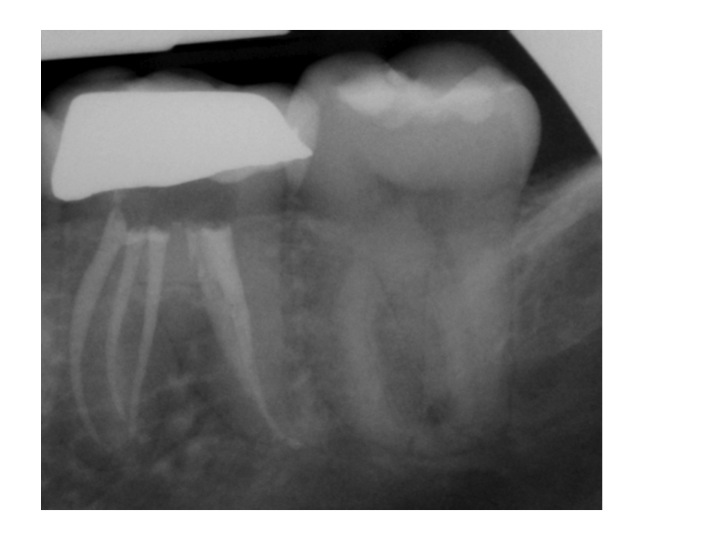
Many methods have been used to study root canal systems in teeth. Dr. Sergio Kuttler has done extensive work with laboratory micro CT imaging, allowing three-dimensional microscopic viewing of an extracted tooth, with a voxel size of about 7 microns (note that a clinical CBCT device will have a voxel size of about 80 microns). Figure 5a shows 3 distinct canals in the mesial root of a mandibular molar. Clinically this phenomenon can be quite elusive; exploration of the isthmus in all mandibular molars is highly recommended. Figure 5b is a preoperative radiograph of tooth #19 on a 28 year-old male of Honduran descent. Of note is the amorphous appearance of the mesial root on the preoperative image. Figure 5c shows the isthmus between the mesial roots. Upon exploration with a #15 hand file, a middle mesial canal was located (Figure 5d). The post- operative radiograph (Figure 5e) shows the cleaned, shaped, and 3 dimensional obturation of 3 canals in the mesial root and 2 canals in the distal root.

5a. Micro CT Mesial root of Mandibular Molar- Courtesy of Dr. Sergio Kuttler

5b. Pre-op #19: Mesial root anatomy appears amorphous.
5c. Isthmus between mesial roots #19
5d. Middle mesial canal with file #19
5e. Post-op #19: Obturation of 3 canals in mesial root of lower molar.
A discussion about isthmuses would not be complete without mention of the C-shaped canal configuration. Figure 6a shows an example of this type of isthmus when seen clinically. These canals present either as a single ribbon-like canal from the orifice to the apex (Figure 6b) or, more commonly, a C-shaped isthmus located on the floor of the pulp chamber that divides into two or three canals with a thin fin-like connection (Figure 6c). 19 Recognition of these configurations facilitates cleaning, shaping, and 3 dimensional obturation, and will maximize the prognosis of the endodontic treatment.
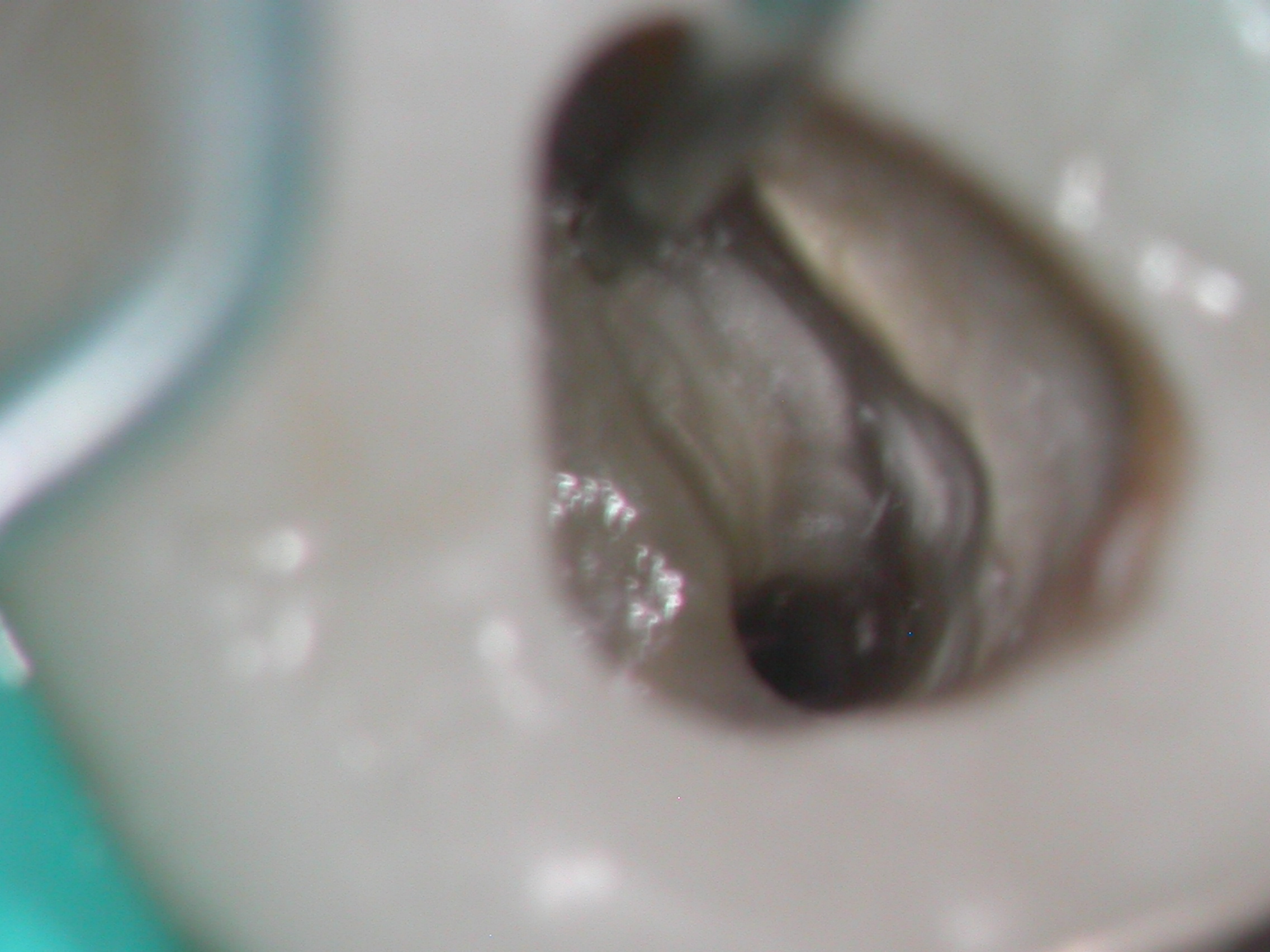
6a. Clinical appearance of C-shaped canal system after access preparation.
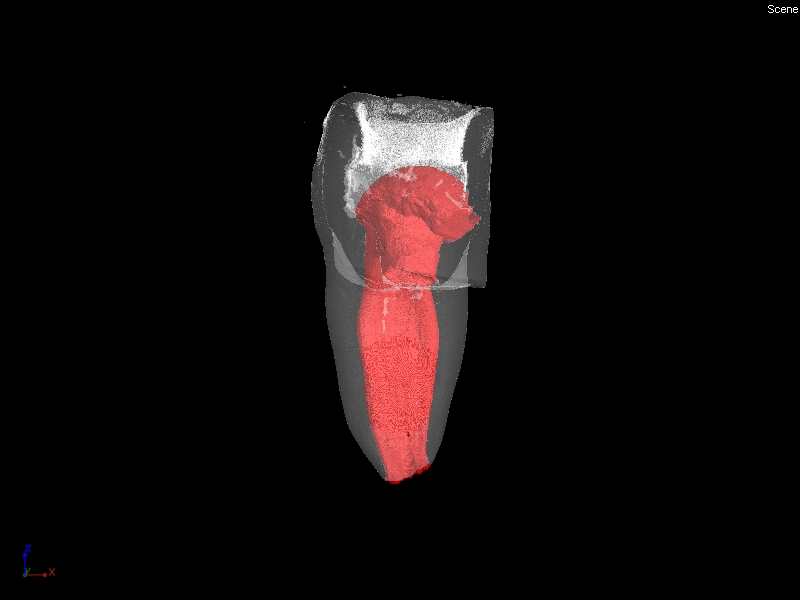
6b. Micro CT of C shaped canal Type 1 in mesial root of a lower molar- Courtesy of Dr. Sergio Kuttler
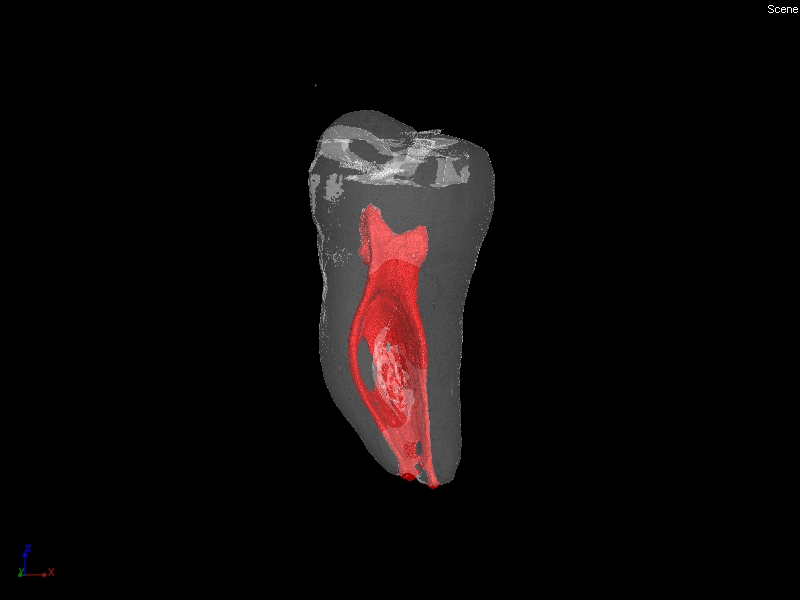
6c. Micro CT of C shaped canal Type 2in mesial root of lower molar- Courtesy of Dr. Sergio Kuttler
Figures 7a and 7b show the pre- and post-operative radiographs of Tooth #18 with a single ribbon-like canal from the orifice to the apex. Figures 8a and 8b are pre- and post-operative radiographs of the more commonly seen “C” shaped configuration whereby there are separate canals that radiate from within the isthmus.

7a. Pre-op #18
7b. Post-op #18: Obturation of a ribbon shaped canal.

8a Pre-op # 31

8b. Post-op #31: Canals diverge initially, yet merge toward
CONCLUSION
Root canal system anatomy has been studied and documented for an entire century. While these studies vary in their findings, the presence of a communication between the canal systems within the individual root is a common observation. Adequate access preparation, exploration of the interior of the tooth with magnification and illumination, and a thorough understanding of anatomic variations in root canal morphology are necessary to perform successful endodontic treatment.
The clinician should pay special attention to the isthmus connecting canals, as its presence makes thorough debridement of the root canal system difficult. Additional canals may originate within this area below the level of the pulp chamber floor. Ultrasonic instruments may be used to trough several millimeters along the isthmus to obtain better access to the tissues associated with the isthmus or any potential hidden canals; however special care must be taken to avoid a perforation in the furcation.
As long as clinical endodontics is performed, the mysteries that lie within the isthmus will be explored both clinically and academically. One thing that is certain: the isthmus is the gift that keeps on giving.
References:
- Hess, W. Formation of root canals in human teeth. The Journal of the National Dental Association, Volume 8, Issues 7-12, 1927;704-725.
- Weller NR, Niemczyk SP, Kim S. Incidence and position of the canal isthmus. Part 1. Mesiobuccal root of the maxillary first molar. Journ of Endod. 1995:21,380–383.
- Vertucci FJ. Root canal anatomy of human permanent teeth, Oral Surg 1984; 58, 589-599.
- Green D. Double canals in single roots. Oral Surg 1973; 35:689-686.
- Pineda F. Roentgenographic investigation of the mesiobuccal root of the maxillary first molar, Oral Surg 1973; 36:253-260.
- Hsu YY, Kim S. The resected root surface: The issue of canal isthmuses. Dent Clin North Am. 1997 Jul; 41(3): 529-540.
- Orban BJ, Bhaskar SN. Orban’s Oral Histology and Embryology; C.V. Mosby, 1991; 86-87.
- Schilder H, DCNA
- Cleghorn BM, Goodacre CJ, Christie, WH, Morphology of teeth and their root canal systems, Ingle’s Endodontics6, Pmph USA; 6 edition (December 31, 2007), p 151-169
- Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgenograpic investigation of 7,275 root canals. Oral Surg 33:101, 1972
- ,Kartal N, Yanikoğlu F., The incidence of mandibular premolars with more than one root canal in a Turkish population., J Marmara Univ Dent Fac. 1992 Sep;1(3):203-10
- Tinelli ME, Ethnic Variations in the Topography of Root Canals, Electronic Journal of Endodontics Rosario, Volume 2, Oct 2011, p 558-562
- Sert S, Bayirli GS, Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. JOE 2004, 30:391-398.
- Benjamin KA, Dowson J, Incidence of two root canals in human mandibular incisor teeth. Oral Surg, Oral Med Oral Path 58(5): 589, 1984.
- Miyashita M, Kasahara E, Yasuda E, Yamamoto A, Sekizawa T. Root canal system of the mandibular incisor. Journal of Endodontics 1997; 23(8):479–484.
- Mauger MJ, Schindler WG, Walker WA 3rd. An evaluation of canal morphology at different levels of root resection in mandibular incisors. Journal of Endodontics 1998; 24(9):607–9.
- Kulid JC, Peters DD: Incidence and configuration of canal systems in the mesiobuccal root of maxillary first and second molars. JOE 16:311, 1990.
- B. Teixeira, C. L. Sano, B. P. F. A. Gomes, A. A. Zaia, C. C. R. Ferraz & F. J. Souza-Filho. A preliminary in vitro study of the incidence and position of the root canal isthmus in maxillary and mandibular first molars International Endodontic Journal, 2003; 36: 276-280
- Jafarzadeh H, Wu YN. J Endod. The C-shaped root canal configuration: a review. 2007 May;33(5):517-23.